There are two pillars of argument against gender-affirming care for youth with gender dysphoria in the reactionary mainstream. These should be instantly familiar to those who have followed the debate over gender-affirming care from any perspective or side, and they are:
1. The increase of transmasculine, female-assigned adolescents with co-occurring mental health issues being referred to gender clinics suggests that some of these children may not really be transgender and could benefit more from therapy instead of transition.
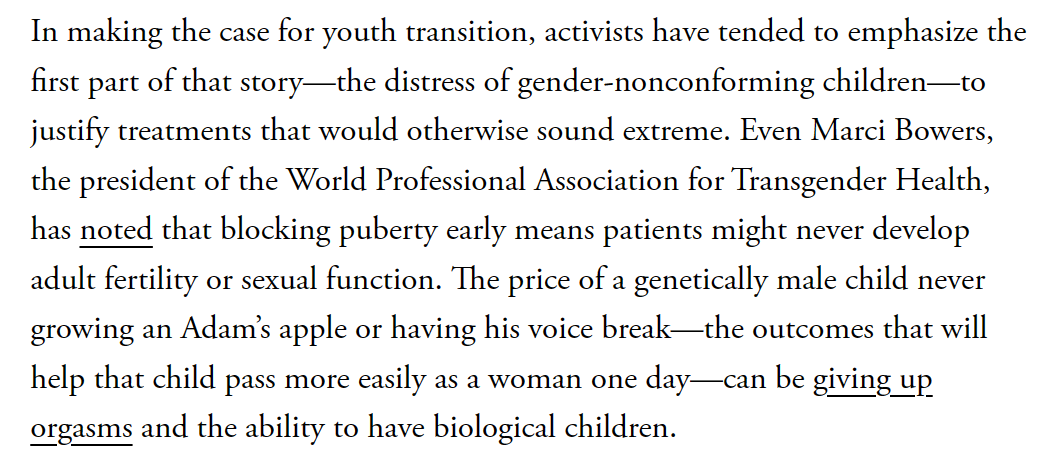
2. The risky, permanent effects of puberty blockers and hormone therapy are such that the merest possibility that some youth patients at gender clinics might not need these drugs constitutes an emergency, a medical scandal the importance and urgency of which it is impossible to overstate.
These two pillars, which appear in every mainstream screed against gender affirming care, were restated again today for the Atlantic by misinformation virtuoso Helen Lewis.
The two pillars are also completely at odds. The risks are to the transfeminine children Lewis agrees show a clear and unambiguous medical need for treatment. Treatments for transmasculine adolescents simply, flatly, do not involve these risks.
Stepping back, let’s first agree, amiably, that if permanent damage was being done to innocent children for no reason, that would be bad. Lewis’ essay positions that common sense perspective against the arguments of Andrea Long Chu, who recently wrote in New York magazine that there should be a human right to change one’s sex that extends to minors. However Chu, in an aside, agreed there are no practical implications to her thesis, saying, “That trans kids’ access to care will in most cases be mediated by parents or legal guardians is an inescapable fact of the way our society regards children, rightly or not.”
Chu’s essay is not particularly interesting, because Chu is not particularly interested in engaging with the fact that children gain the intellectual and emotional competence to make informed decisions gradually. The vulnerability and inexperience that childhood imposes makes grand rhetoric granting children the right to change sex akin to rhetorically granting them the right to sprout wings and fly. Lewis, for her part, seems equally uninterested in Chu, spending most of the article arguing against the position that Chu didn’t take, that gender-affirming medical interventions for youth are infrequent, carefully weighed, and evidence based. That’s the position I hold, and the one Lewis’ misinformation is designed to undermine, with Chu as a sideshow.
Returning to our two pillars, Lewis states pillar one thus:
“What kicked off the current debate was a steep rise in the number of children seeking care, and the changing demographics of those children. In recent years most of the patients have been genetically female, and many of them presented with other issues, such as autism, eating disorders, anxiety, or past trauma.”
In other words, according to Lewis herself, the rise in transmasculine youth seeking care is at the very heart of her objections to gender-affirming care for youth.
The second pillar, that gender-affirming care is too risky due to its permanent effects, is stated no less clearly, in one of Lewis’ opening paragraphs.
Taken together, the inference is clear: Lewis and other critics are saying that the problem with gender-affirming care is that medical risks which are appropriate for trans girls who exhibit clear signs of gender dysphoria from early childhood are not appropriate for transmascs whose gender dysphoria comes on at puberty, particularly if it is combined with other signs of mental distress.
What it leaves out, the bait and switch that Lewis and her ilk rely on their audience not realizing, is that the risks for these two groups of patients are not the same. To the extent that there are permanent, non-cosmetic risks to fertility, sexual function, and bone density in early interventions for gender dysphoric youth, those risks are to transfeminine youth who receive puberty blockers in early puberty, then progress to hormone therapy and surgery. These are the same patients the evidence shows are overwhelmingly likely to grow up to be transgender girls, and for whom undergoing an unwanted masculinizing puberty would constitute a serious risk to their social and mental wellbeing.
The other, newer group? Transmasculine youth who present at gender clinics in adolescence who Lewis and others insist are the reason people in the mainstream ought to feel alarm over the practices of gender clinics? There is no evidence whatsoever that their fertility, sexual function, or bone density is at any risk at all. Instead, the risk of an erroneous transition for a transmasculine person is primarily the risk of detransition: That wanted changes such as beard growth or voice deepening could become unwanted later on. However, research has repeatedly shown that such transition regret is very rare.
So, why are we having this moral panic again?
Misinformation peddlers like Lewis rely on the reputation of outlets like the Atlantic, combined with bad faith debating tactics that obscure the realities of gender-affirming care. The good news, which Lewis does not want you to know, is that the most serious, most frequently-touted risks of early intervention in trans youth apply only to transfemmes with early, persistent, and insistent gender dysphoria. Fortuitously, this is the exact group for whom the risks are most likely to be outweighed by the benefits to their social and emotional health. Meanwhile, the risks to adolescents of either sex who don’t block puberty in the earliest stages are low. These risks do not seem to include permanent damage to fertility or ability to orgasm. If such youth are more likely to desist (and there is no evidence whatsoever that they are), we can rest easy knowing they are less at risk for the serious harms people like Lewis claim to be so worried about.
Mainstream opponents of gender-affirming care have big platforms at journalistic stalwarts, and they are bolstered by the background bigotry and prejudices of ordinary people, who often find transness a little weird. However, they do not have the scientific evidence on their side, instead relying on cherry-picking and sleight-of-hand. They do not have the plainspoken, honest truth. The impressive lengths people like Lewis go to to obscure the true picture of gender-affirming care, including which risks apply to which groups of patients, demonstrates just how little such people care for truth and honest debate.
Evan Urquhart is a journalist and the founder of Assigned Media.




I read Lewis’s article with a growing sense of unease and outrage. Thank you for this response, which I wish the Atlantic would publish to rebut her claims. Probably wishful thinking, but it would be the right and fair thing to do.