
In 2020, in the UK, in an atmosphere of increasing political anger and animosity directed at the transgender community, pediatrician Hilary Cass was tasked with reviewing the state of gender-affirming care for youth by the NHS. The Final Report of the Cass Review, released on April 9th, is a 388-page document that almost immediately became the center of gravity in the ongoing political debate about how and whether to treat young people with gender dysphoria. The Report made international news and has been taken as vindication by many anti-trans activists.
A document that approaches four hundred pages will be difficult for most people to read in full, meaning that inevitably most of the public will be forced to rely on summaries provided by journalists, commentators, activists, and others. This article seeks to provide a brief but comprehensive summary for Assigned Media’s audience.
The Cass Review vs the Cass Report
Dr. Cass served as the chair of the independent Cass Review and, for four years, sought data and information pertaining to the treatment of gender diverse children and adolescents in the NHS. While it is clear that others collaborated with Cass, and at least one member of the advisory board has been identified, it remains unclear who the board consisted of.
The Review comissioned a series of studies from the University of York, in England. These included systematic reviews of the evidence on treatments for gender dysphoria in youth, a survey of European youth gender clinics, an investigation of treatment guidelines, a quantitative study of the youth seen by the GIDS clinic in England, and a qualitative study of young people, parents, and clinicians’ attitudes and thoughts on treatment. The Report relies in part on this material, although it includes many other sources of information and in some places lapses into speculation with no clear evidentiary basis.
The Cass Report includes summaries of some of the results of the York research in its 12 appendices, including summaries of the qualitative and quantitative studies of the GIDS program.
Weak Evidence for All Interventions
A systematic review collects all the published research in an area and ranks the research based on how likely it is to be reliable. The weakest form of evidence are case reports, where a doctor formally writes up an anecdote about a patient. The strongest form of evidence are randomized controlled trials where patients are randomly assigned to some type of medication or intervention, or to no intervention, or to a placebo, and the groups are compared to see how an intervention compares to alternatives/no treatment/placebo. Systematic reviews of several interventions for trans youth were undertaken by the University of York including puberty blockers, cross sex hormones, social transition, and psychosocial support measures.
The results of each of the systematic reviews was to characterize the overall evidence as weak, which was the Report’s most significant finding and has been widely reported. When looking more granularly at the York papers, a pattern appears of some papers showing a psychological benefit of the intervention, a smaller number showing no change positive or negative, and no papers showing any psychological harm. For example, in the systematic review of the evidence on puberty blockers, several included studies suggested psychological benefits to treatment in a range of areas, while a smaller number of studies found no significant impact. This was summarized in both the papers and the Report as “weak evidence” but could also be accurately described as weak evidence favoring treatment.
No evidence for any alternative treatment approach to gender dysphoria was included. Although one of the systematic reviews examined psychosocial interventions, none of the included studies looked at psychosocial interventions offered as substitutes for medical treatments.
Speculation On Causes of Trans Identity
The Cass Report also devoted many pages to consideration of the possible causes for transgender identity. It included a summary of twin studies, which have provided mixed evidence, with two studies finding that gender identity likely had a genetic component, and one study finding that uterine environment might be a stronger influence. However, the Report seems to downplay these possibilities in favor of speculation that transgender identity is caused by social factors, while stressing a mix of factors was likely.
One chain of reasoning speculated that social transition and/or medical treatment might cause or solidify a transgender identity in someone who might otherwise not be transgender. To the extent that this was based in any sort of evidence, the Report made much of the fact that most people with intersex conditions identify with their “sex of rearing,” meaning that they do not subsequently transition.
Sex of rearing is a near-perfect synonym of sex assigned at birth. While the Report implies the “sex of rearing” of transgender youth is somehow related to social transition, this is not accurate. Transgender children are reared in their birth-assigned gender. It is the tension or difference between a person’s assertion of their gender identity and their sex of rearing that defines a transgender identity.
The report also mentions the possibility that gender dysphoria in youth could be caused by trauma or other mental illness. There is no evidence provided on this.
Suggestion that Trans Identity Development is a Harm of Treatment
The Report’s speculation about the causes of transgender identity lead directly into speculation that young patients who are allowed to socially or medically transition may be influenced to become transgender when they might otherwise not have been. The Report consistently treats this possibility very seriously indeed, and treats it as self-evident that it would be a harm of any treatment if a child who might otherwise not have been transgender develops a transgender identity. It does not provide any direct support or rationale for this, nor does it provide evidence of any other harm of treatment, although the possibility that height and bone density might be impacted by puberty blockers is also mentioned.
Evidence from the GIDS Service in England
Less of the Report than might be expected deals with the Review’s findings on the young patients who were served by the GIDS service and their outcomes. Appendix 8 (page 329) of the Report details these findings. The Report found 73 percent of youth referred to the clinic were transmasculine/female assigned and 27 percent were transfeminine/male assigned.
(The report consistently refers to patients by their birth-assigned sex, and is particularly insistent in using information about adolescent girls as the reference point for discussing the transmasculine population. The terms “transgender boy” and “transgender girl” do not appear anywhere in the Report, nor does “transmasculine,” “transfeminine,” or any term describing a young trans person’s gender that would normally be considered respectful by the transgender community. The word nonbinary appears several times, and the words “transgender man” and “transgender woman” appear twice each, on page 90.)
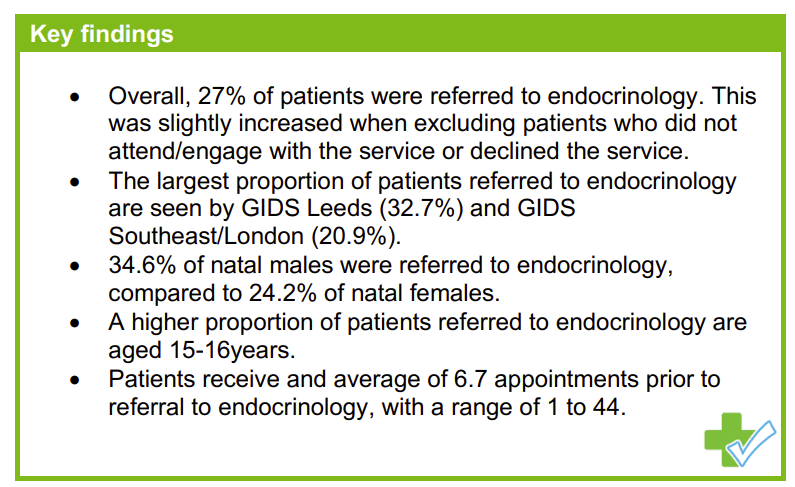
The Report found very few youth referred to GIDS received hormone blockers or cross sex hormones. Only 27 percent of youth referred to GIDS were referred to endocrinology, with 82 percent of those receiving puberty blockers, often at the age of 15 or 16 suggesting irreversible changes from puberty were well underway before a blocker was available. Of those who were not referred to endocrinology, 69 percent were referred on to adult gender services, suggesting large numbers of youth aging out while on the waiting list.
No evidence of youth being rushed into treatment was found, with most receiving five or six appointments before an endocrinology referral. However, the Report found poor note-taking and inadequate recordkeeping by GIDS of the type of assessments that led to a referral.
The Report found fewer than 10 examples of detransition in 3306 patient records with enough information to be included in the audit.
Cass Report Recommendations
The Report included many recommendations for treatment of youth presenting at gender clinics in England. Some of these were fairly technical, describing proposed relationships between NHS entities such as regional centers, centralized authorities, and local/tertiary providers. Other recommendations were broader. These included the recommendation to provide more psychosocial interventions, to explore all non-medical treatment options, to treat social transition as a serious intervention that might lead to a transgender identity, to prohibit puberty blockers outside of a research study, and limit the provision of cross-sex hormones to the rarest of cases. The recommendations synthesize a view of medical transition as a bad outcome to be avoided, and a belief that gender dysphoria can be successfully treated non-medically, despite no non-medical interventions being evaluated in any of the series of systematic reviews that found weak evidence in favor of puberty blockers, cross-sex hormones, social transition, and psychosocial support for young people on waiting lists or undergoing medical interventions.
Evan Urquhart is the founder of Assigned Media and an incoming member of the 2024-2025 Knight Science Journalism fellowship class at MIT.




